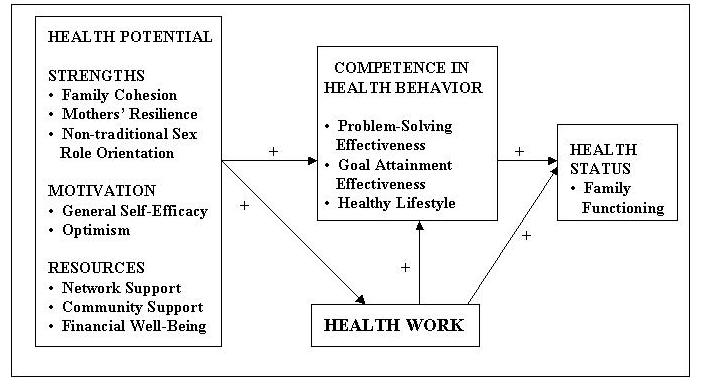
Figure 1. Causal Model of Single-Parent Family Health Promotion.
TESTING A
CAUSAL MODEL OF FAMILY HEALTH PROMOTION BEHAVIOUR
IN MOTHER-HEADED SINGLE-PARENT FAMILIES
Study Purposes
The purpose of this study was to test a causal
model derived from the Developmental Health Model (Allen, 1994; Ford-Gilboe, 1997a, 1998)
in a diverse sample of female-headed single-parent families with school-age children.
Conceptual Framework
The Developmental Health Model (DHM)(Allen,
1994; Ford-Gilboe, 1998; DeMarco, Ford-Gilboe, et al, 2000) provides a vehicle for
understanding how the potential within families and their members contributes to their
participation in health promotion processes (i.e. health work) and, over time, the
outcomes of this participation on lifestyle and functioning. The Developmental Health
Model (DHM) is a theoretical extension and refinement of the McGill Model of Nursing, a
curriculum model first developed by Moyra Allen and faculty at the McGill University
School of Nursing in the 1970's. A causal model derived from selected concepts in the DHM
was tested in this study (Figure 1).
Additional Research Questions:
1. How do demographic and contextual variables influence health potential, health work and
health outcomes?
2. What are the similarities and differences between subgroups of SPFs on the main study
and demographic variables?
3. How do single mothers describe critical aspects of health promotion behaviour and
strengths in the context of their lives?
Figure 1. Causal Model of Single-Parent Family Health
Promotion.
Methodology
Design
Cross-sectional, comparative survey
Family interviews were also used to validate and enrich quantitative findings by enhancing interpretation, and to provide new insights into the role of contextual factors in health promotion of single-parent families.
Sample and Setting
A non-random, convenience sample of 236 single-parent families was recruited from a
mid-size Ontario city. Single-parent families were eligible to participate if the mother
had been raising at least one school-age child (between the ages of 5-14) on her own for a
minimum of one year, was unmarried and not cohabitating and was fluent in English.
Measures
Eleven of the 13 study variables were measured using reliable and valid summated rating
scales. The two remaining variables, problem-solving effectiveness and goal-attainment
effectiveness, were measured using single visual analogue scales using accepted guidelines
for VAS construction, administration and scoring (Lee & Kieckhefer, 1989).
Summary of Main Findings
* Results of structural equation modelling (SEM) using AMOS in SPSS Windows suggested a
good fit of the model and the data, suggesting that the health potential of single-parent
families positively affects their competence in health behaviour both directly and
indirectly, through the process of health work, and that these changes result in enhanced
family functioning.
* Mother's internal capabilities (resilience, general self-efficacy, optimism) held the strongest relationships with health work while resources held among the weakest. Thus, the personal strengths of single mothers are critical to healthy family outcomes.
* Neither legal marital status or route to single-parenthood provided a meaningful way of differentiating subgroups of SPFs who varied in their capacities and functioning.
* Being employed was associated with many positive outcomes for single mothers, particularly their resilience, community support and financial well-being.
Health
Promotion in Single-parent Families
Home Page
Last updated on XX/XX/XX by Dr.
Marilyn Ford-Gillboe .
Web Design: Jeff Morrison